MRI_subacute_hemorrhage
MRI_subacute_hemorrhage_T1W
MRI_subacute_hemorrhage_T2W
MRI_subacute_hemorrhage_FLAIR
MRI_subacute_hemorrhage_GRE
MRI of Hemorrhage in the Brain
Author: William G. Bradley, MD, PhD, FACR
Objectives: Upon the completion of this CME article, the reader will be able to
1. Describe the different types of hemoglobin and what makes them paramagnetic or diamagnetic.
2. Describe the different stages of hemorrhage into the parenchyma of the brain in regard to magnetic resonance appearance and why the appearance changes over time.
3. Discuss the magnetic resonance appearance of nonparenchymal hemorrhage and the sensitivity of MRI regarding the detection of these types of bleeds.
Introduction
Magnetic resonance imaging (MRI) is more sensitive than x-ray computed tomography (CT) in detecting hemorrhage in the brain parenchyma, and the intraventricular, subdural, or subarachnoid spaces. Compared to CT, MRI is also more specific in determining the age of hemorrhage in the brain. Using a combination of T1- and T2-weighted images, MRI can distinguish five stages of hemorrhage: hyperacute (intracellular oxyhemoglobin), acute (intracellular deoxyhemoglobin), early subacute (intracellular methemoglobin), late subacute (extracellular methemoglobin), and chronic (hemosiderin rim surrounding proteinaceous heme derivatives known as “hemichromes”).
Figure 1 demonstrates the oxidative denaturation of hemoglobin. When blood comes out of the lungs fully oxygenated, it is in the oxyhemoglobin form in which a molecule of oxygen (O2) is attached at the sixth coordination site of the heme iron. When blood goes through the capillary circulation, it gives off its oxygen, thus forming deoxyhemoglobin (in which case there is nothing at the 6th coordination site of the heme iron). In both oxy and deoxyhemoglobin, the heme iron is in the reduced, ferrous, Fe++ state in order to be able to transfer oxygen back and forth. When removed from the high oxygen environment of the circulation, some metabolic pathways (for example, the enzyme methemoglobin reductase) fail, allowing the heme iron to become oxidized to the ferric Fe+++ form, which is called methemoglobin. Although methemoglobin has both an acid form and a base form, the acid form (in which a water molecule is attached to the heme iron (figure 1) predominates at normal physiologic pH. Continued oxidative denaturation of methemoglobin leads to hemichromes in which a histidine molecule from the globin chain becomes attached to the 6th coordination site of the heme iron.
Whether the heme iron is oxidized or reduced has everything to do with its ability to transfer oxygen but has absolutely nothing to do with its MR appearance. The MR appearance depends on whether the heme iron has unpaired electrons or not. When there are unpaired electrons, the nucleus is said to be “paramagnetic”, in which case marked T1 or T2 shortening may be seen. Deoxyhemoglobin has four unpaired electrons and methemoglobin has five. (This compares with seven unpaired electrons on the intravenous MR contrast agent, gadolinium.) In chronic hemorrhage, blood breakdown products are absorbed by macrophages and are turned into hemosiderin, which is also paramagnetic. The oxyhemoglobin in hyperacute hemorrhage and the hemichromes in chronic hemorrhage have no unpaired electrons and are said to be “diamagnetic”.
Parenchymal Hemorrhage
Table I summarizes the time course and MR appearance of the five stages of parenchymal hemorrhage on T1- and T2-weighted MR images. Hyperacute hemorrhage (intracellular oxyhemoglobin) has a longer T1 and a longer T2 than brain due to its higher water content. This will cause it to appear relatively dark on a T1-weighted image and bright on a T2-weighted image. Unfortunately, this is the same pattern of signal intensity seen in any edematous mass (for example, an abscess, tumor, or acute demyelination). Almost immediately, deoxyhemoglobin is formed at the periphery of a hyperacute hematoma where it is in contact with actively metabolizing brain (figure 2). As noted above, deoxyhemoglobin is paramagnetic and, when it is inside an intact red cell, it creates a non-uniform magnetic environment, which causes pronounced T2 shortening. This appears dark on a T2-weighted MR image. (This low signal is best seen on the b=0 image of an EPI diffusion technique, followed by a T2*-weighted gradient echo image, followed by a T2-weighted conventional spin echo image, and is least best seen on a T2-weighted fast spin echo image.) The low intensity “deoxyhemoglobin border” of hyperacute hemorrhage tends to be somewhat irregular and may even be incomplete (figure 2). It is typically surrounded by bright vasogenic edema on a T2-weighted image. Both of these features distinguish a deoxyhemoglobin border from the hemosiderin rim seen in chronic hematomas.
Table I: Stages of Parenchymal Hemorrhage
Stage Time Compartment Hemoglobin T1 T2
Hyperacute < 24 hrs. Intracellular Oxyhemoglobin Medium Medium
Acute 1 to 3 days Intracellular Deoxyhemoglobin Long Short
Subacute – Early 3 + days Intracellular Methemoglobin Short Short
Subacute – Late 7 + days Extracellular Methemoglobin Short Long
Chronic – Center 14 + days Extracellular Hemichromes Medium Medium
Chronic – Rim 14 + days Intracellular Hemosiderin Medium Short
Over the subsequent 24 hours, the hematoma turns dark throughout on a T2-weighted image because all of the oxyhemoglobin is converted to deoxyhemoglobin as the hematoma becomes “acute” (figure 3). The T1 relaxation time of an acute hematoma is longer than that of brain; therefore, acute hematomas are also dark on T1-weighted images (although not nearly to the degree that they are on T2-weighted images – figure 4).
Approximately three days after hemorrhage, the hematoma will begin to turn bright at the margins on T1-weighted images as deoxyhemoglobin is converted to methemoglobin. As long as the red cells are intact, however, this area will remain dark on T2-weighted images, because intracellular methemoglobin has a short T2 (figure 5). Both intracellular deoxyhemoglobin (acute hemorrhage) and intracellular methemoglobin (early subacute hemorrhage) appear dark because both have paramagnetic heme iron inside of the intact red cells. Because of this paramagnetism, the inside of the red cell becomes more magnetized than the nonparamagnetic plasma on the outside of the red cell. This leads to magnetic non-uniformity, which causes dephasing, or T2 shortening, and thus decreased signal on a T2-weighted image.
Approximately one week following hemorrhage into the brain parenchyma, the red cells in the hematoma begin to break down. With hemolysis, the paramagnetic methemoglobin gets mixed with the nonparamagnetic plasma, eliminating magnetic non-uniformity and T2 shortening. Since the water content of a late subacute hematoma is greater than that of brain, the T2 relaxation time is prolonged and the hematoma is now bright on a T2-weighted image.
Both intracellular and extracellular methemoglobin are bright on T1-weighted images. This is due to the fact that water can diffuse freely across the red cell membrane. Therefore, whether the red cells are intact or not, water can easily get to the paramagnetic heme iron with subsequent T1 shortening. Notice in Table I that the only hemoglobin with a short T1 that is bright on a T1-weighted image is methemoglobin.
After approximately two weeks, macrophages appear at the borders of the parenchymal hematoma and begin to convert the extracellular methemoglobin to hemosiderin and ferritin. Both of these substances are paramagnetic and lead to T2 shortening. This produces a dark hemosiderin ring around the rest of the hematoma, identifying the chronic stage (figure 6). It should be stressed that macrophages only start digesting blood breakdown products after the red cells have lysed; they will not attack intact red cells. Thus, extracellular methemoglobin will always be noted subjacent to the hemosiderin rim.
Early in the chronic stage, bright, extracellular methemoglobin is noted centrally on both T1- and T2-weighted images. Gradually, this is further oxidized to Hemichromes, which are proteinaceous but not paramagnetic. This causes minor T1 shortening compared to brain tissue but not nearly to the degree seen with paramagnetic methemoglobin. Gradually over the next year or two, the liquid center of the chronic hematoma is resorbed, leaving only the hemosiderin rim. This remains forever like a tattoo of the brain.
Nonparenchymal Hemorrhage
The times in Table I apply primarily to parenchymal hematomas; hemorrhage into the extra-axial, intraventricular, or subarachnoid compartments evolves more slowly because the oxygen tension in these compartments is higher (maintaining the methemoglobin reductase system longer). While subacute subdural hematomas are notoriously isodense to brain on CT, there is no form of hemorrhage that is isointense to brain on both T1- and T2-weighted images in MR. While chronic subdural hematomas and subdural hygromas (i.e., CSF collections in the subdural space due to an arachnoid rent) often have a low density appearance by CT, these are easily distinguished by MR on the basis of the higher protein content in the chronic subdural hematoma. This leads to slightly higher signal on T1-, proton density-, and T2-weighted images (and much higher signal intensity on FLAIR images).
FLAIR, which is a heavily T2-weighted image with cerebral spinal fluid (CSF) nulling based on its T1 relaxation time, is also an excellent technique for diagnosing acute subarachnoid hemorrhage. In this case, the sensitivity is based on the protein content of the serum, which shortens the T1 of the CSF so it is no longer nulled, making it bright and easily detectable (figure 7). In two studies from Japan in the mid 1990s, FLAIR was shown to be 100% sensitive for the detection of subarachnoid hemorrhage (compared to CT). In our own laboratory, we’ve performed phantom experiments demonstrating that FLAIR is two orders of magnitude more sensitive than CT for the detection of acute subarachnoid hemorrhage. This great sensitivity to acute subarachnoid hemorrhage coupled to the “deoxyhemoglobin border” sign of hyperacute hematomas will ultimately allow MRI to replace CT for the detection of acute hemorrhage in patients with stroke.
Figures
1 A schematic showing the oxidative denaturation of hemoglobin.
2 Deoxyhemoglobin border in a hyperacute hemorrhage approximately 10 minutes following bleeding. The key finding is the low signal partial deoxyhemoglobin border surrounding the hyper-intense oxyhemoglobin on the T2 weighted image (right side).
3 Acute hematoma – in a T1-weighted image, the hematoma is dark.
4 Acute hematoma – in a T2-weighted image, the hematoma is even darker.
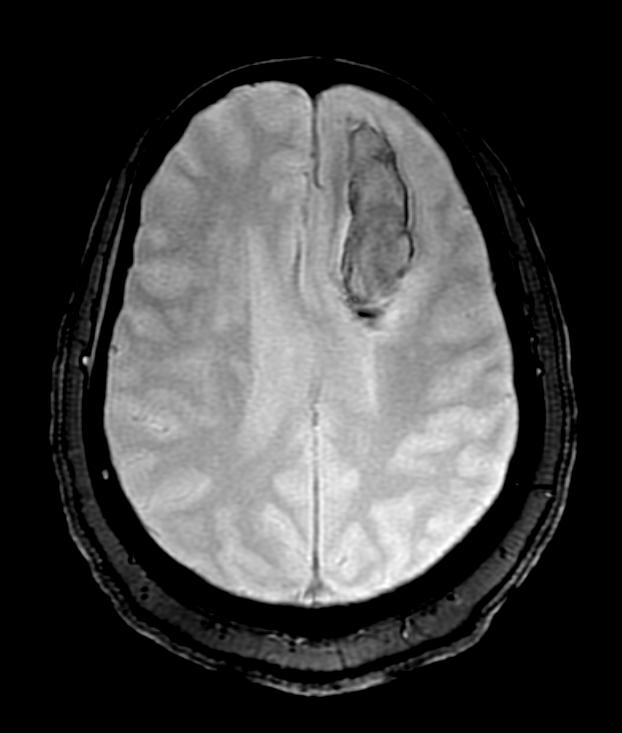
5 An early subacute hemorrhage is bright on a T1-weighted image (left) turning dark on a T2-weighted image (right).
6 A chronic hematoma in the right thalamus with surrounding dark hemosiderin rim on the T2-weighted image. The bright late subacute hemorrhage (extracellular methemoglobin) in the center will be slowly resorbed over several years.
7 Acute Subarachnoid hemorrhage on FLAIR. Normally cerebral spinal fluid (CSF) is dark on FLAIR (as noted in the ventricles). With T1 shortening from the protein in the serum, the CSF is now bright on FLAIR (i.e. in the sulci).
References or Suggested Reading:
1. Bradley WG, Schmidt PG. “Effect of methemoglobin formation on the MR appearance of subarachnoid hemorrhage” Radiology 156:99-103, 1985.
2. Gomori JM, Grossman RI, Goldberg HI, et al. “Intracranial hematomas: imaging by high field MR” Radiology 1985;157:87-92.
3. Bradley WG. Chapter 58 “Hemorrhage” in Stark DD, Bradley WG (eds) Magnetic Resonance Imaging, 3rd ed (Mosby-Yearbook, St. Louis, MO), 1999.
4. Bradley WG. “MR appearance of hemorrhage in the brain” Radiology 1993;189:15-26.
5. Atlas SW, Thulborn KR. “MR detection of hyperacute parenchymal hemorrhage of the brain: AJNR 1998;19(8):1471-7.
6. Noguchi K, Ogawa T, Inugomi A, et al. “Acute subarachnoid hemorrhage: MR imaging with fluid-attenuated inversion pulse sequences” Radiology 1995;196:773.
7. Noguchi K, Ogawa T, Inugomi A. “MR of acute subarachnoid hemorrhage: preliminary report of fluid attenuated inversion recovery pulse sequences” AJNR 1994;15:1940.
About the Author:
Dr. William Bradley currently is the director of the Magnetic Resonance Imaging Center at Long Beach Memorial Medical Center, in Long Beach, California. He is also a Professor of Radiology at the University of California, Irvine. He actively teaches Magnetic Resonance Imaging to medical students, Radiology residents and fellows in Radiology.
Dr. Bradley has over 100 publications in peer-review journals and is actively involved in research in the field of Magnetic Resonance Imaging. He has presented his research and has given lectures on MRI topics at major conferences around the country as well as internationally, including Europe, Japan, and India.
Examination:
1. A hemosiderin rim surrounding proteinaceous heme derivatives is known as
A. deoxyhemoglobin
B. ferritin
C. hemichromes
D. methemoglobin
E. ferrous sulfate
2. When blood comes out of the lungs fully oxygenated, it is in the oxyhemoglobin form in which a molecule of oxygen (O2) is attached at the _______ coordination site of the heme iron.
A. second
B. third
C. fourth
D. fifth
E. sixth
3. When blood goes through the capillary circulation, it gives off its oxygen, thus forming
A. deoxyhemoglobin
B. oxyhemoglobin
C. hemosiderin
D. methemoglobin
E. ferritin
4. In both oxy and deoxyhemoglobin, the heme iron is in the reduced, ______ state in order to be able to transfer oxygen back and forth.
A. ferric
B. ferrous
C. ferritin
D. methemoglobin
E. hemichrome
5. Continued oxidative denaturation of methemoglobin leads to hemichromes in which a _________ molecule from the globin chain becomes attached to the 6th coordination site of the heme iron.
A. ferric
B. ferritin
C. ferrous
D. histidine
E. carbon
6. Whether the heme iron is oxidized or reduced has everything to do with
A. its ability to transfer oxygen.
B. its MR appearance.
C. its ability to transfer heme.
D. its CT appearance.
E. its ability to transfer carbon.
7. The MR appearance depends on whether the heme iron has
A. unpaired neutrons or not.
B. paired electrons or not.
C. unpaired electrons or not.
D. paired neutrons or not.
E. unpaired protons or not.
8. Which of the following statements is true?
A. When there are unpaired electrons, the nucleus is said to be “diamagnetic”, in which case marked T1 or T2 lengthening may be seen.
B. When there are paired electrons, the nucleus is said to be “paramagnetic”, in which case marked T1 or T2 shortening may be seen.
C. Deoxyhemoglobin, methemoglobin, and hemosiderin are “diamagnetic”.
D. The intravenous MR contrast agent, gadolinium, has five unpaired electrons.
E. The oxyhemoglobin in hyperacute hemorrhage and the hemichromes in chronic hemorrhage have no unpaired electrons and are said to be “diamagnetic”.
9. A hyperacute hemorrhage (with its intracellular oxyhemoglobin) has a higher water content than the surrounding brain tissue, which causes it to appear
A. relatively bright on a T1-weighted image and bright on a T2-weighted image. B. relatively dark on a T1-weighted image and bright on a T2-weighted image. C. relatively dark on a T1-weighted image and dark on a T2-weighted image.
D. relatively bright on a T1-weighted image and dark on a T2-weighted image. E. relatively isointense on a T1-weighted image and dark on a T2-weighted
image.
10. Almost immediately following a hyperacute hemorrhage, _________ where it is in contact with actively metabolizing brain.
A. hemosiderin is formed at the periphery
B. ferritin is formed at the periphery
C. methemoglobin is formed at the periphery
D. deoxyhemoglobin is formed at the periphery
E. oxyhemoglobin is formed at the periphery
11. The two features that distinguish a deoxyhemoglobin border from the hemosiderin rim seen in chronic hematomas are
A. that it is usually fairly complete and regular and it is typically surrounded by dark vasogenic edema on a T2-weighted image.
B. that it is usually fairly complete and regular and it is typically surrounded by bright vasogenic edema on a T2-weighted image.
C. that it is somewhat irregular or may even be incomplete and it is typically surrounded by dark vasogenic edema on a T2-weighted image.
D. that it is somewhat irregular or may even be incomplete and it is typically surrounded by bright vasogenic edema on a T2-weighted image.
E. that it is usually fairly complete and regular and it is typically surrounded by bright vasogenic edema on a T1-weighted image.
12. Regarding the acute stage of a brain hemorrhage,
A. the timing of this is 7 + days
B. there is intracellular methemoglobin
C. the T1 is long and the T2 is short
D. there is extracellular hemichromes
E. the T1 is medium and the T2 is short
13. Regarding the chronic stage of a brain hemorrhage,
A. the center has a medium T1 and a medium T2
B. the center has extracellular methemoglobin
C. the rim has intracellular methemoglobin
D. the rim has a long T1 and a medium T2
E. the timing is considered 7 + days
14. Which of the following statements is true?
A. Over the subsequent 24 hours from a bleed, the hematoma turns dark throughout on a T2-weighted image because all of the deoxyhemoglobin is converted to oxyhemoglobin as the hematoma becomes “acute”.
B. The T1 relaxation time of an acute hematoma is shorter than that of brain; therefore, acute hematomas are also dark on T1-weighted images.
C. Approximately three days after hemorrhage, the hematoma will begin to turn dark at the margins on T1-weighted images as oxyhemoglobin is converted to methemoglobin.
D. Because the red cells are lysed in an “acute” hemorrhage, the area will remain dark on T2-weighted images, because of extracellular methemoglobin.
E. Both intracellular deoxyhemoglobin (acute hemorrhage) and intracellular methemoglobin (early subacute hemorrhage) appear dark because both have paramagnetic heme iron inside of the intact red cells.
15. Which of the following statements is true?
A. With hemolysis, the diamagnetic methemoglobin gets mixed with the paramagnetic plasma, eliminating magnetic non-uniformity and T2 shortening.
B. Since the water content of a late subacute hematoma is greater than that of brain, the T2 relaxation time is prolonged and the hematoma is now bright on a T2-weighted image.
C. Both intracellular and extracellular methemoglobin are dark on T1-weighted images.
D. Whether the red cells are intact or not, water can easily get to the diamagnetic heme iron with subsequent T1 shortening.
E. The only hemoglobin with a short T1 that is bright on a T1-weighted image is deoxyhemoglobin.
16. Which of the following statements is strue?
A. After approximately two weeks, macrophages appear at the borders of the parenchymal hematoma and begin to convert the extracellular deoxyhemoglobin to methemoglobin.
B. Both hemosiderin and ferritin are paramagnetic and lead to T2 shortening.
C. The T2 shortening caused by hemosiderin and ferritin produces a bright hemosiderin ring around the rest of the hematoma, identifying the chronic stage.
D. Macrophages only start digesting blood breakdown products with intact red cells; they will not attack red cells that have been lysed.
E. Extracellular deoxyhemoglobin will always be noted subjacent to the hemosiderin rim.
17. Gradually over the next year or two following a brain hemorrhage, the liquid center of the chronic hematoma is resorbed, leaving only the _______, which remains forever like a tattoo of the brain.
A. hemosiderin rim
B. ferrous rim
C. ferric rim
D. ferritin rim
E. methemoglobin rim
18. Which of the following statements is (are) true?
A. Hemorrhage into the extra-axial, intraventricular, or subarachnoid compartments evolves more slowly because the oxygen tension in these compartments is lower.
B. While subacute subdural hematomas are notoriously isointense to brain on T1-weighted and T2-weighted MRI, there is no form of hemorrhage that is isodense to brain on CT.
C. While chronic subdural hematomas and subdural hygromas often have a low density appearance by CT, these are easily distinguished by MR on the basis of the higher protein content in the chronic subdural hematoma.
D. A & B above.
E. B & C above.
19. FLAIR is also an excellent technique for diagnosing _______ because the protein content of the serum shortens the T1 of the CSF so it is no longer nulled, making it bright and easily detectable.
A. subacute hygromal hemorrhage.
B. subacute subdural hemorrhage.
C. chronic subdural hemorrhage.
D. acute subarachnoid hemorrhage.
E. chronic subarachnoid hemorrhage.
20. In the two studies discussed in this article from Japan performed in the mid 1990s, FLAIR was shown to be ______ sensitive for the detection of subarachnoid hemorrhage (compared to CT).
A. 75%
B. 80%
C. 90%
D. 95%
E. 100%